






Mental health policies exist across nearly every healthcare system, yet access to care remains far more limited than those policies suggest. In 2021 alone, one-third of people living with mental illness and nearly half of those with serious conditions were unable to receive treatment. Behind well-intentioned legislation, administrative barriers quietly erode care quality and restrict who actually gets help.
The consequences extend far beyond individual patients. Mental health issues cost the U.S. economy an estimated $225 billion each year through medical expenses and lost productivity. At the same time, structural incentives push providers away from accessible care. Nearly half of psychiatrists refuse insurance altogether, compared to just 20% of other specialists, largely because in-network mental health services pay roughly half as much as out-of-network care.
The system is also strained by provider burnout. At a time when approximately 50% of clinicians reported burnout due to insufficient staffing and excessive workload, in the first year of the COVID-19 pandemic, that number rose to 76%. Medicaid patients are most affected, with only 35% of psychiatrists willing to take on new Medicaid patients, compared to 62% willing to take on either Medicare or private insurance.
How Administrative Barriers Undermine Mental Health Policy Goals
The administrative processes intended to facilitate the delivery of mental health services have grown to be more hindrances than facilitators, limiting the ability of patients to obtain the mental health services they require. Many healthcare administration articles have documented that bureaucracy has undermined otherwise well-intentioned mental health policy by transforming potential solutions into actual barriers to care for both patients and providers.
Disconnect Between Policy Intent and Practice Reality
A stark reality exists between what policies aim to achieve and what happens on the ground. Only 46% of US adults with mental illness got specialised mental health treatment in 2020, despite laws meant to make treatment more accessible. Several factors create this gap:
- Complex paperwork: Lengthy forms, document requirements, and face-to-face interviews create major hurdles
- Divided systems: Mental health care remains separate from regular medical care, which makes integration difficult
- Knowledge gaps: Many people don’t know which benefits they can get or how to apply for them
The disconnect grows deeper because regulators often lack insight into the challenges healthcare providers face daily. Rules that seem logical on paper become impractical in actual clinical settings.
Impact on Access to Mental Health Care for Medicaid Patients
Medicaid patients feel the weight of these administrative barriers the most. Medicaid pays for most mental health care in the US, yet its reimbursement rates fall below those of Medicare and private insurance. This explains why only 46% of psychiatrists take new Medicaid patients, while 75% accept Medicare patients.
Checking eligibility adds another layer of difficulty. Regular income reviews flag households for small changes, and their coverage could stop if they don’t quickly provide proof documents. Even short breaks in coverage lead to more hospital stays, fewer doctor visits, and rising medical bills.
The stress of navigating the mental health system causes patients to become frustrated. When patients are unsure of what is required for eligibility, they lose faith in the government services that provide mental health coverage and will eventually give up on getting covered again. This can cause individuals to lose interest in obtaining mental health treatment because this goes directly against the overall intent of mental health policy.
Credentialing and Contracting Delays in Insurance Networks
Insurance credentialing creates major roadblocks when mental health providers try to join provider networks. These administrative hurdles affect patient care quality and work against broader mental health policy goals.
Multi-Month Onboarding Timelines for Mental Health Providers
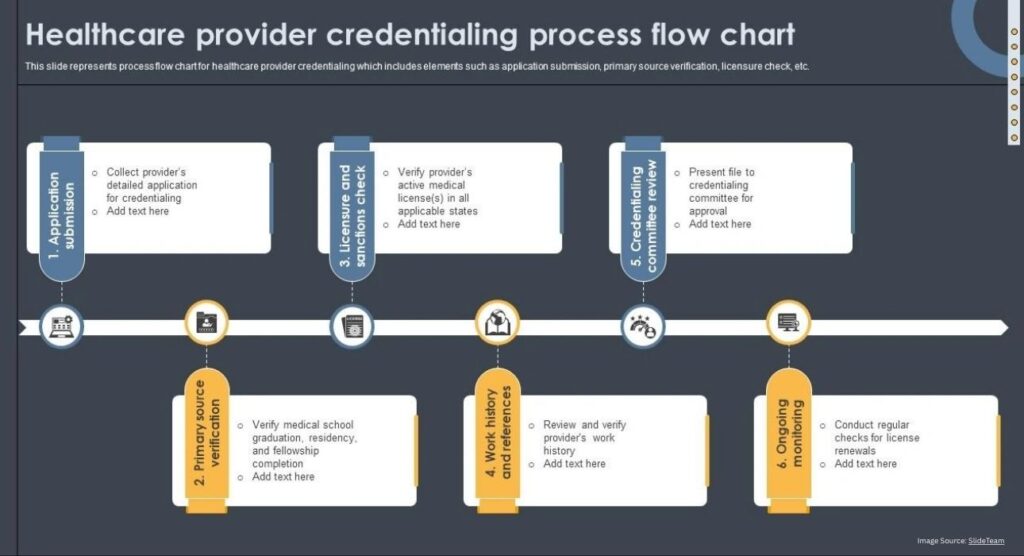
Mental health providers must wait months before they can help insured patients. Insurance companies say it takes about 90 days to process applications. The reality looks quite different. Credentialing usually takes between 60 and 120 days after providers submit their applications. Some providers wait nearly four months. These delays hit providers hard financially. A new therapist waiting 90 days to get approved loses about $45,000 in billable sessions they could have provided.
Variation in Documentation Across Health Plans
Providers face a heavy burden when they try to join networks. Each credentialing application needs:
- Complete verification of licenses, educational records, malpractice coverage, and detailed work histories
- Special requirements just for mental health providers, such as telehealth rules and supervision records
- Custom paperwork that fits each payer’s specific forms and requirements
Even tiny paperwork mistakes can lead to more delays or rejected applications. Different rules from each payer create confusion and errors. Providers waste time as they customize applications for every insurer.
Third-Party Oversight in Managed Care Models
Managed care adds another complex layer to the process. Many insurers let outside companies handle customer service. This limits how well representatives can help providers with their concerns. A former Cigna manager pointed out that overseas staff often can’t access full claims systems and don’t understand complex medical terms well. This maze of bureaucracy sometimes seems deliberate—making the process “so frustrating for providers to follow up on claim denials, they’re just going to give up, and the insurance company is not going to have to pay out”. Today, all but one of these psychologists (48%) say administrative challenges like pre-authorisation requirements and audits stop them from taking insurance.
Claims Processing and Reimbursement Challenges
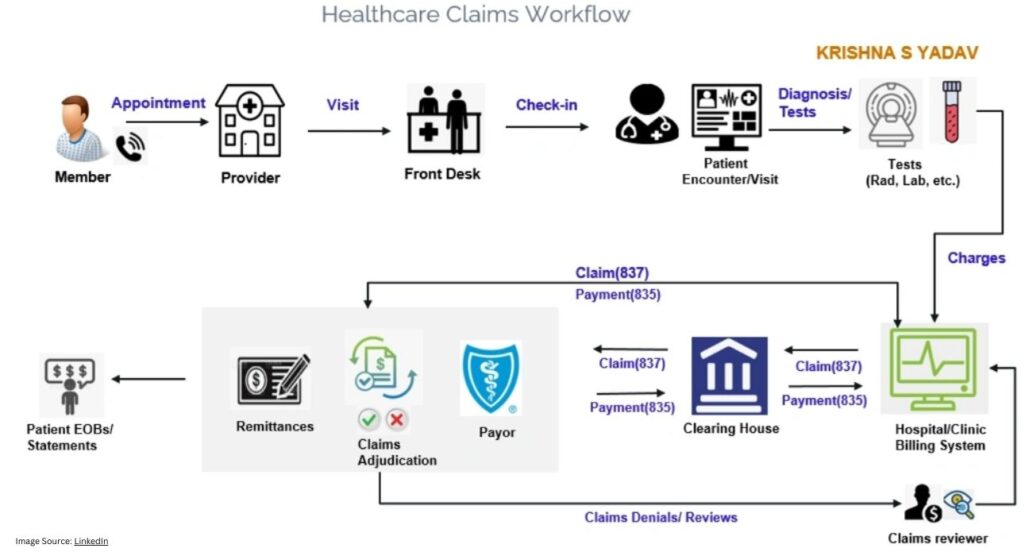
Mental health providers experience significant frustration due to technical challenges when trying to bill for their services. Often, technical issues experienced by providers create barriers to obtaining reimbursement for their services. The barriers to reimbursement create financial pressure on providers and limit patients’ ability to access quality mental health services.
Coding Limitations for Co-occurring Disorders
Mental health coding creates many barriers for the providers. Providers have difficulty capturing the full clinical picture of their patients when multiple conditions coexist. Missing important information, such as nicotine dependence with withdrawal, can significantly lower the reimbursement rate for the patient. Documentation for mental health requires a significant amount of detail—basic documentation, such as “supportive therapy was provided”, often does not meet the medical necessity requirements and leads to denied claims.
Prior Authorisation for Substance Use vs Mental Health Services
Insurance companies create uneven access to services through their authorisation requirements. These measures delay essential treatment. Substance use disorder treatments usually skip requirements that still apply to mental health services. This gap persists even though 90% of doctors say authorisation processes hurt patient care.
Revenue Loss from Denials and Resubmissions
These challenges hit practices hard financially. Behavioural health practices see denial rates 50-85% higher than other medical specialities. Reworking each denied claim costs $25-100, and insurance companies reject 30% of behavioural health claims on first submission. About 65% of denied claims are never resubmitted, resulting in permanent revenue loss. These burdens explain why 34% of psychologists avoid insurance networks.
Systemic Reforms to Improve Care Quality and Access
New technologies and optimised processes are effective ways to overcome administrative barriers to mental health care. These breakthroughs can fix systemic problems without overhauling existing policies.
Federal Standardisation of Billing Eligibility
Better documentation standards could cut down administrative waste. Traditional Medicare’s improper payments reached 7.66%, costing $31.70 billion annually. Almost 60% of these errors are due to poor documentation. Mental health providers deal with different coding rules from various payers. Federal programs that create uniform billing requirements would help reduce these mistakes.
Express Access Programs and Real-Time Credentialing
The NIH-funded Express Access Network shows promising results in making provider enrollment easier. This platform uses scientific algorithms to match patients with providers and boosts recovery rates up to 5 times. Real-time credentialing tools speed up verification by checking licenses, certifications, and sanctions databases automatically. These tools help providers start practising and billing sooner.
Reducing Compliance Costs Through Process Automation
AI-powered automation helps mental health practitioners handle their documentation load. Doctors spend almost 6 hours each day working with electronic health records. Automation tools turn lengthy documentation into quick review tasks instead of manual data entry. AI-driven billing systems also cut down claim denials by checking codes against regulations.
Conclusion
Administrative barriers silently affect mental health care outcomes. While policy aims to increase access to mental health care, bureaucratic processes limit a patient’s ability to choose their provider, delay treatment, and add additional cost burdens to the patient. Providers are also affected by administrative barriers, including burnout from long credentialing times and low reimbursement rates. Those who are most vulnerable (especially Medicaid recipients) experience the largest gaps in access to mental health services.
If no changes occur, the current administrative barriers will continue to increase the treatment gap, even with increased coverage of all individuals under the Affordable Care Act. Some solutions to the administrative barriers include using standardised billing systems, streamlining the credentialing process, and automating many tasks that currently require significant manual intervention and review.





Leave feedback about this